Understanding Incident-To Billing Through the Special Investigations Unit Lens

Understanding Incident-To Billing Through the Special Investigations Unit Lens
Incident-to billing remains one of the most misunderstood and frequently scrutinized billing practices in healthcare fraud, waste, and abuse (FWA). While it is designed to support efficient, team-based care delivery, incident-to billing presents high-risk visibility gaps that can obscure true rendering providers, supervision practices, and care accountability.
When viewed through the Special Investigations Unit (SIU) lens, incident-to billing comes into sharper focus, revealing both its value and its risks. In the FWA space, incident-to billing is a recurring source of referrals, audits, and recoveries. The very structure of incident-to billing, allowing services performed by non-physician practitioners (NPPs) to be billed under a physician’s National Provider Identifier NPI, creates opportunities for misrepresentation of rendering provider, inflated reimbursement, and concealment of supervision deficiencies.
Understanding how incident-to billing operates in practice, is essential for identifying actionable FWA risk.
What is Incident-to Billing?
Incident-to billing is a Medicare-specific provision that allows certain follow-up services performed by nurse practitioners (NPs) or physician assistants (PAs) to be billed under a supervising physician’s NPI, provided specific requirements are met. When applied correctly, it can improve efficiency and support coordinated care.
However, its complexity makes it a frequent target for SIU review. Accurate documentation, proper supervision, and strict adherence to Centers for Medicare & Medicaid Services (CMS) requirements are essential to ensure compliance and reduce risk. Because payer policies may vary, providers must also understand and follow payer-specific expectations.
Regulatory Framework
Incident‑to billing and related supervisory requirements operate within a strict federal regulatory structure. To ensure compliant billing, providers must understand and follow CMS rules, HIPAA documentation standards, and federal fraud and abuse laws.
💡SIUs must interpret these rules as elements of proof when evaluating potential FWA.
The sections that follow explore the key requirements, risk indicators, and investigative considerations that shape how incident-to billing is evaluated in practice.
CMS Requirements
SIUs should assess whether the following elements can be substantiated with evidence, not just stated in documentation:
Initial Visit Restriction: Documentation reflects the physician evaluated new patients or any new condition and established the treatment plan. Non‑physician practitioners (NPPs) cannot independently create or modify the plan.
Non‑Institutional Setting: Incident‑to billing is limited to office-based settings and is not permitted in institutional environments, such as hospitals or skilled nursing facilities (SNFs). An SIU investigation must determine whether services occurred in the appropriate setting.
Direct Supervision: Prior to 2026, direct supervision required the physician to be physically present in the office and immediately available. Beginning in 2026, supervision may be provided through real-time, two-way audio, and video technology (excluding audio only communication). However, global surgical services continue to require in‑person supervision. Investigators must ask, “Was the physician actually available at the time of service?”
Employment and Scope of Practice: Both the supervising physician and the NPP must be employed by the same billing entity, and the NPP must operate within their state-defined scope of practice. From an SIU perspective, this element should be supported by employment records, credentialing files, and applicable licensure or delegation requirements to determine whether the billing relationship was valid and whether services were furnished within lawful authority.
Type of Service: Incident-to billing is limited to office-based professional services and does not apply to diagnostic services, durable medical equipment (DME), or services that fall under separate Medicare benefit categories. SIUs should evaluate whether the service billed was eligible for incident-to treatment or whether the claim reflects category misuse that created improper reimbursement exposure.
FWA Exposure and Legal Risk
From an SIU enforcement perspective, incident-to violations often escalate beyond billing errors into false claims exposure. Improper incident-to billing may involve:
Upcoding or overbilling
Misrepresentation of rendering provider
Billing for services not rendered under required supervision
💡Key Investigative Insight: Single claim errors are rarely escalated in isolation. SIU exposure increases when repeated documentation gaps, supervision failures, or rendering-provider inconsistencies form a broader pattern tied to financial impact.
In this context, incident-to billing risk is not limited to technical noncompliance. When unsupported claims are repeated over time, the issue may shift from billing error to a broader pattern of false representation and repayment exposure.
Special Investigation Unit Oversight and Detection Activities
SIUs should use data analytics, documentation review, and pattern analysis to identify activities that may indicate improper billing or supervision. Through an analytical lens, SIUs examine patterns, behaviors, and documentation to uncover risks that may not be immediately visible.
Key Risk Indicators SIUs Review:
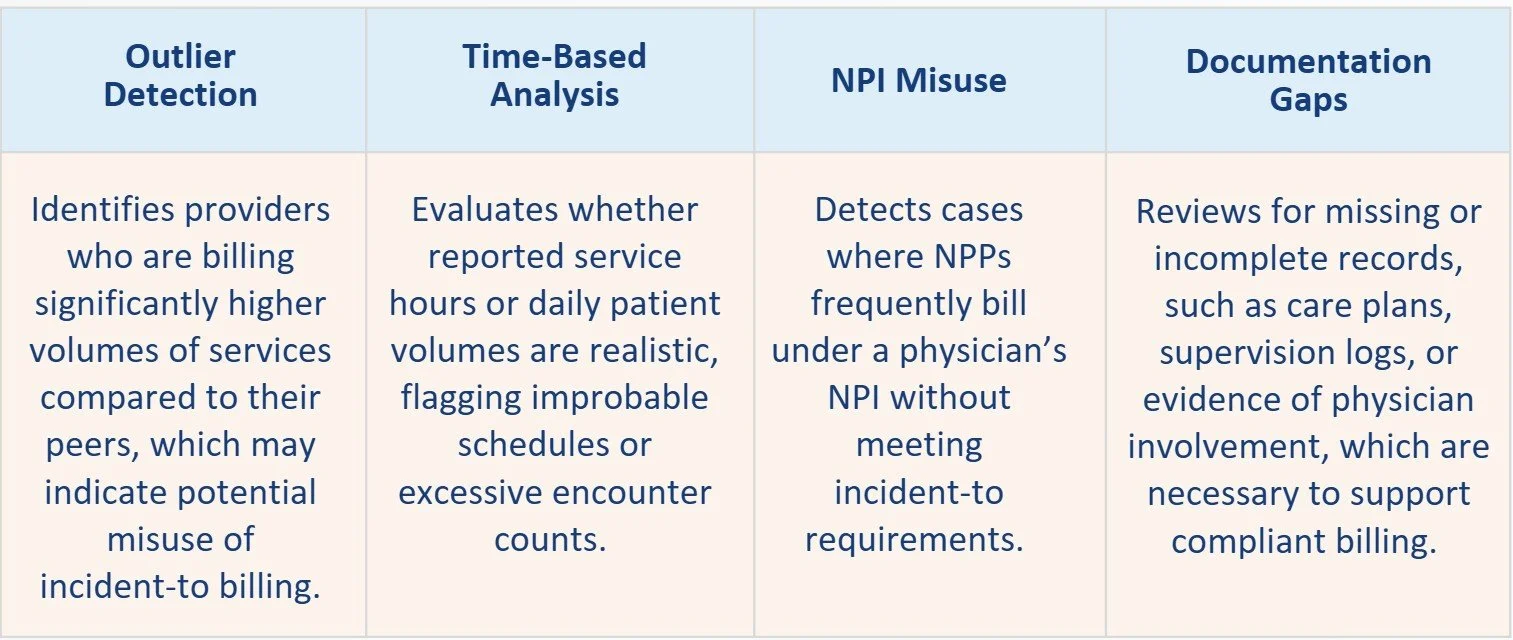
💡These indicators help bring potential compliance concerns into focus, highlighting where closer review may be needed.
What SIUs Need to Build a Case
SIUs and auditors rely on documentation to verify who performed each service, confirm appropriate supervision, and ensure all billing criteria are met.
Documentation reviews should include:
Medical Records: Physician-authored initial visit; ongoing link to established plan of care
Supervision Evidence: Logs identifying the supervising physician; documentation of whether supervision was provided onsite or virtually
Operational Records: Provider schedules; staffing rosters; clinic coverage logs
Encounter Data: Rendering provider vs. billing provider comparison
Governance Materials: Internal incident-to policies; training materials; supervision protocols
💡Key SIU Principle: If supervision or physician involvement cannot be independently validated, it is NOT defensible.
Common Investigative Scenarios
Phantom Physician Involvement: A physician is listed as the supervising provider across all claims, but no schedule overlap exists and no documentation confirms presence.
SIU Interpretation: Potential false representation of supervision to obtain higher reimbursement.
NPP-Driven Practices Billing at Physician Rates: A clinic’s operations are largely driven by NPs/PAs, yet nearly all claims bill under a physician NPI.
SIU Interpretation: Systemic misuse of incident-to billing to maximize revenue.
Institutional Setting Misuse: Services in SNFs or hospitals billed as incident-to.
SIU Interpretation: Clear policy violation with high recovery potential due to identifiable claim sets.
Recommended Policy Enhancements for Payers
To reduce incident-to FWA exposure, payers should:
Require rendering provider transparency on claims
Deploy analytics targeting supervision feasibility
Implement prepayment edits for high-risk POS codes
Conduct focused audits on high-volume physician NPIs
Align policies with clear, enforceable documentation standards
💡Together, these measures create a structured framework that improves consistency, strengthens oversight, and brings expectations into clearer focus.
Conclusion
Incident-to billing presents a unique challenge for SIUs: it is legitimate in structure but vulnerable in execution. From an FWA investigative perspective, the risk lies not in the policy itself, but in its ability to:
Obscure who performed the service
Mask supervision failures
Facilitate higher reimbursement through misrepresentation
💡SIUs serve as a critical control point, leveraging data, documentation, and investigative expertise to ensure billing integrity and protect payer resources.
Integrity Advantage is Here to Help
Whether it is conducting FWA program assessments, strengthening internal processes, or providing outsourced SIU support, Integrity Advantage partners with healthcare organizations nationwide to turn insights into action. Together, we help teams move from goals to measurable progress. Integrity Advantage is a certified Women’s Business Enterprise (WBE) and Woman Owned Small Business (WOSB).
With more than 30 years of experience supporting payers, the team at Integrity Advantage provides healthcare fraud, waste and abuse consulting, outsourced investigations and medical record reviews for Special Investigations Units and other organizations fighting healthcare fraud. We are a certified Women’s Business Enterprise (WBE) and an Economically Disadvantaged Woman Owned Small Business (EDWOSB).
For more information click below, call us at 866-644-7799 or email info@integrityadvantage.com.